
How a $5 Pack of Abortion Pills in Ethiopia Sparked a Movement to ‘Demedicalize’ Access in the U.S.
In her new book, Access, Rebecca Grant chronicles activists' decades-long fight to defy abortion restrictions—including the origin story of Plan C.
Photo: Getty Images AbortionBooks
This is an excerpt from Access: Inside the Abortion Underground and the Sixty-Year Battle for Reproductive Freedom, by Rebecca Grant. The book chronicles activists’ decades-long mission to defy abortion restrictions and fight for reproductive freedom, from the U.S. to France, Mexico, the Netherlands, and more.
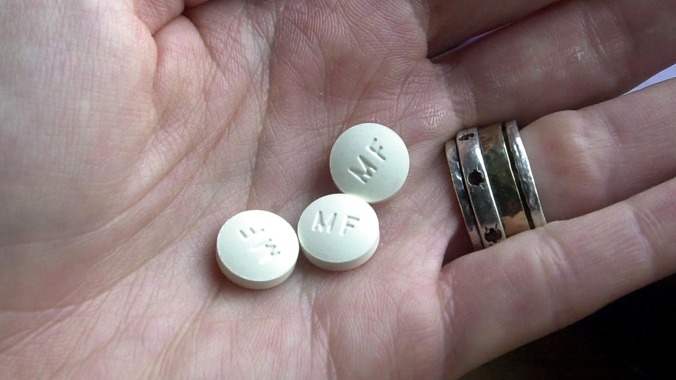
In 2014, Elisa Wells and Francine Coeytaux were positioned outside a pharmacy in Ethiopia waiting for a colleague to come out. The pharmacy was sandwiched between two stores with green signs that read “Fujifilm Digital Print Shop” and set back from the bustling red-and-yellow sidewalk. A few moments later, their companion, a woman, emerged holding a box. White and light brown with a yellow rose and branded as a “Safe-T” kit, its label read: “This pack contains treatment for early medical abortion.”
Wells and Coeytaux were stunned. There they were in the Ethiopian highlands, in one of the poorest, most health-challenged countries in the world, and people could walk into a pharmacy and buy a combination pack of abortion pills, including mifepristone and misoprostol. In the United States, FDA regulations only allowed mifepristone to be dispensed within the confines of a clinic, medical office, or hospital, making it no easier to access than surgical abortion; it wasn’t available in pharmacies, nor could it be sent in the mail, even by certified prescribers. Also, there were no “medical termination of pregnancy” (MTP) kits, also known as “combipacks,” available in the US, in which the appropriate dosages of mifepristone and misoprostol were packaged together in one blister pack, as was available elsewhere. (American patients received each of the two medications in separate packaging.)
Moreover, a medication abortion in the US cost around $500–600, while the kit the woman was holding, with generic versions of the same medications, had cost around $5. That was expensive by local standards, but the gap in price was still hard for Wells and Coeytaux to wrap their minds around.
They were part of a team for the MacArthur Foundation evaluating projects that used misoprostol to treat postpartum hemorrhage in sub-Saharan Africa. Observing the availability of medication abortion kits in the region— how available they were, how relatively easily they could be obtained directly by patients, how the distribution of the medication was community-based instead of rooted in a medical system—threw into sharp relief how not just burdensome but also superfluous the hurdles were in the US.
Back home, conversations around the People’s Filibuster and the passage of HB2 [in Texas] had been churning, and the women thought about how “beyond ridiculous” it was that abortion pills were easier to obtain in remote parts of sub-Saharan Africa than in Texas. Given that US clinics were under attack from TRAP laws, that traveling to clinics posed a challenge for many patients, and that there was an abundance of international evidence that medication abortion could be safely and effectively administered in outpatient settings, then surely it made sense to explore models for abortion access that didn’t have an in-person visit to a clinic at the center. They had no illusions that freeing the medication from its regulatory constraints would be easy, but they were determined to try.
Over the years, a handful of American groups had worked doggedly to make medication abortion more widely accessible and to encourage the FDA to relax its burdensome requirements, but all in all they had made little progress. Frustrated by the bureaucratic intransigence, and concerned about the future of abortion rights, a smaller cohort had begun meeting over the years to discuss self-managed abortion. In 2004, Susan Yanow, who was then involved with Women on Waves, had convened a “Misoprostol Alone Working Group,” and between 2009 and 2011, she conducted trainings on misoprostol in the Rio Grande Valley in Texas. In 2009, Gynuity Health Projects—which had been founded in 2003 by Beverly Winikoff, a doctor and researcher who had worked at the Population Council for twenty-five years—and the Reproductive Health Technologies Project hosted a meeting to discuss the legal issues of using misoprostol for abortion outside the legal system. Then, in 2013, Yanow and Marlene Gerber Fried held a secret summit about self-managed abortion with misoprostol, put on by Hampshire College’s Civil Liberties and Public Policy Program, in response to the new laws in Texas, and later that year, there was another meeting in D.C. about “how to ensure that women in the US have the information, resources, and support they need to use abortion pills safely.” But while there may have been ongoing discussions about self-managed abortion, there wasn’t a dedicated organization in the US that was actively and openly sharing practical information about it. Determined to change that, Wells and Coeytaux teamed up and started laying the groundwork for Plan C, a nonprofit dedicated to supporting direct, unimpeded, “demedicalized” access to medication abortion, advocating for looser restrictions on mifepristone through the regulated pathways, and sharing resources around self-managed abortion. (Most of the work on self-managed abortion at the time focused on misoprostol because mifepristone was so hard to come by.)
Their first step was to map the existing landscape. One of Wells’s prevailing questions had to do with the accessibility of misoprostol outside of official channels: Did a black market for abortion pills exist in the US? Was it possible to buy them online? Assisted by Victoria Nichols, the daughter of a close friend of Coeytaux’s, Wells sleuthed around the internet, typing in search terms in English and Spanish: “get abortion pills now,” “get abortion pills cheap,” “where can I find abortion pills,” “can I get abortion pills online.” They dug deep into the search results and, a few pages down, discovered websites that purported to sell medication abortion regimens. Then, Wells stumbled upon a Yahoo chat room where people discussed how they’d bought pills online and which pharmacy websites they’d used; she also unearthed FDA records that contained complaints against websites that sold illicit abortion pills, and checked to see if any of those websites were still active. Some were. Equipped with those early findings, Wells and Nichols conducted a second, more systematic search and assembled a comprehensive list. After bringing all the information together, in 2014 they wrote a report called “Surfing for Abortion” about their experience, and although it was never published, they presented the findings to their colleagues and used it as a blueprint for moving forward.
Wells continued to monitor the landscape, and around 2016 she noticed that MTP kits containing both mifepristone and misoprostol, like she’d seen in Africa, were becoming available online through unregulated vendors. Again, she gathered the URLs of the sites, but this time she decided to buy the medication and see what happened. The kit cost a few hundred dollars, and Wells was nervous that her payment information would be stolen—the website was rudimentary, and the interface felt sketchy—but in the end she felt it was worth the risk. She entered her address and payment details, and then she waited. A week or so later, she was sitting in her home office and spotted her mail carrier coming up the driveway with a package. She walked outside, signed for it, and went back inside her house to open it. It was her order of abortion pills.
Wells posted on Facebook about her experience, and James Trussell, a professor she knew from the emergency contraception campaign, saw the post and suggested she talk to Elizabeth Raymond at the research group Gynuity. Raymond, too, was interested in learning more about the unofficially sourced medication. They decided to collaborate on an experimental project to purchase abortion pills from sixteen different websites and then send them to a lab to have them tested, curious if the pills were what they purported to be.
As it turned out, they were. Of the pills they received in the mail, five different manufacturers were represented, mostly generics from India. Some of the pills had shipped from abroad, but to their surprise, a majority of the packages originated from within the US—the first package Wells ordered had a return address in Colorado. Entrepreneurs, it seemed, were buying cheap medication in India and sneaking it into the US in suitcases, or receiving shipments of medication from pharmacy partners in India and hoping they did not get intercepted by customs; then they were reselling the medications at a markup through simple websites with names like “Abortion Pills RX.” While they sold the pills for way more than they had cost to purchase in India, the price tag was still less than medication abortion in a clinic, and came with the added convenience of ordering online and receiving the package at home. Payment generally happened via wire transfer or Western Union.
Wells and Coeytaux were impressed that the medications were legitimate, but the online vendors offered limited communication and minimal, if any, guidance on the appropriate protocol for using the pills. The process was transactional and lacked options for practical or emotional support that feminist groups like Women on Web, Women Help Women, and Las Libres provided. Still, the medication was as advertised, which meant there was a channel where people could safely end their pregnancies without needing to engage with the medical system or leave their homes in the US. This was significant, especially given the growing interest in self-managed abortion. In 2015, Wells and Coeytaux had heard of new research from the Texas Policy Evaluation Project of the University of Texas at Austin that estimated that somewhere between 100,000 and 240,000 women in Texas alone had tried to self-manage their abortions. Because of the clinic closures in the wake of HB2 and the state’s proximity to the border, Texas was unique, but there was anecdotal evidence to suggest the phenomenon was occurring in other states as well.
Excited by their findings, Wells, Coeytaux, and a third cofounder, Amy Merrill, reconceived Plan C as a digital hub for sharing information about medication abortion and self-managed abortion. Coeytaux cited the activists behind the Del-Em as an inspiration, building off the idea that abortion didn’t have to be a medical event presided over by doctors, but could be something laypeople with the right tools handled independently.
From ACCESS by Rebecca Grant. Copyright © 2025. Reprinted by permission of Avid Reader Press, an Imprint of Simon & Schuster, Inc.
Like what you just read? You’ve got great taste. Subscribe to Jezebel, and for $5 a month or $50 a year, you’ll get access to a bunch of subscriber benefits, including getting to read the next article (and all the ones after that) ad-free. Plus, you’ll be supporting independent journalism—which, can you even imagine not supporting independent journalism in times like these? Yikes.